
Inferior oblique muscle
| Inferior oblique | |
|---|---|
 Rectus muscles: 2 = superior, 3 = inferior, 4 = medial, 5 = lateral Oblique muscles: 6 = superior, 8 = inferior Other muscle: 9 = levator palpebrae superioris Other structures: 1 = Annulus of Zinn, 7 = Trochlea, 10 = Superior tarsus, 11 = Sclera, 12 = Optic nerve | |
 Sagittal section of right orbital cavity. | |
| Details | |
| Origin | Orbital surface of the maxilla, lateral to the lacrimal groove |
| Insertion | Laterally onto the eyeball, deep to the lateral rectus, by a short flat tendon |
| Artery | Ophthalmic artery |
| Nerve | Oculomotor nerve |
| Actions | Extorsion, elevation, abduction |
| Identifiers | |
| Latin | musculus obliquus inferior bulbi |
| TA98 | A15.2.07.019 |
| TA2 | 2051 |
| FMA | 49040 |
| Anatomical terms of muscle | |
The inferior oblique muscle or obliquus oculi inferior is a thin, narrow muscle placed near the anterior margin of the floor of the orbit. The inferior oblique is one of the extraocular muscles, and is attached to the maxillary bone (origin) and the posterior, inferior, lateral surface of the eye (insertion). The inferior oblique is innervated by the inferior branch of the oculomotor nerve.
Structure
[edit]The inferior oblique arises from the orbital surface of the maxilla, lateral to the lacrimal groove. Unlike the other extraocular muscles (recti and superior oblique), the inferior oblique muscle does not originate from the common tendinous ring (annulus of Zinn).
Passing lateralward, backward, and upward, between the inferior rectus and the floor of the orbit, and just underneath the lateral rectus muscle, the inferior oblique inserts onto the scleral surface between the inferior rectus and lateral rectus.
In humans, the muscle is about 35 mm long.[1]
Innervation
[edit]The inferior oblique is innervated by the inferior division of the oculomotor nerve (cranial nerve III).
Function
[edit]Its actions are extorsion, elevation and abduction of the eye.
Primary action is extorsion (external rotation); secondary action is elevation; tertiary action is abduction (i.e. it extorts the eye and moves it upward and outwards). The field of maximal inferior oblique elevation is in the adducted position.
The inferior oblique muscle is the only muscle that is capable of elevating the eye when it is in a fully adducted position.[2]

Clinical significance
[edit]While commonly affected by palsies of the inferior division of the oculomotor nerve, isolated palsies of the inferior oblique (without affecting other functions of the oculomotor nerve) are quite rare.
"Overaction" of the inferior oblique muscle is a commonly observed component of childhood strabismus, particularly infantile esotropia and exotropia. Because true hyperinnervation is not usually present, this phenomenon is better termed "elevation in adduction".[3]
Surgical procedures of the inferior oblique include: loosening (also known as recession see Strabismus surgery), myectomy, marginal myotomy, and denervation and extirpation. It is also encountered and identified in lower lid blepharoplasty surgeries.
Additional images
[edit]-
 Eye movement of lateral rectus muscle, superior view
Eye movement of lateral rectus muscle, superior view -
 Eye movement of medial rectus muscle, superior view
Eye movement of medial rectus muscle, superior view -
 Eye movement of inferior rectus muscle, superior view
Eye movement of inferior rectus muscle, superior view -
 Eye movement of superior rectus muscle, superior view
Eye movement of superior rectus muscle, superior view -
 Eye movement of superior oblique muscle, superior view
Eye movement of superior oblique muscle, superior view -
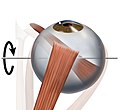
 Eye movement of inferior oblique muscle, superior view
Eye movement of inferior oblique muscle, superior view -
 Anterior view
Anterior view







-
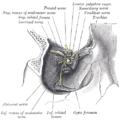 Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure.
Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure. -
 Inferior oblique muscle
Inferior oblique muscle -
 Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection. -
 Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection.




References
[edit]![]() This article incorporates text in the public domain from page 1023 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 1023 of the 20th edition of Gray's Anatomy (1918)
- ^ Riordan-Eva, P (2011). Vaughan & Asbury's General Ophthalmology (18th ed.). New York: McGraw-Hill Medical. ISBN 978-0071634205.
- ^ "Eye Theory". Cim.ucdavis.edu. Archived from the original on 2014-05-27. Retrieved 2012-12-07.
- ^ Kushner BJ (2006). "Multiple mechanisms of extraocular muscle 'overaction'". Arch Ophthalmol. 124 (5): 680–8. doi:10.1001/archopht.124.5.680. PMID 16682590.
External links
[edit]- Anatomy figure: 29:01-08 at Human Anatomy Online, SUNY Downstate Medical Center
- lesson3 at The Anatomy Lesson by Wesley Norman (Georgetown University) (orbit5)
- Image at childrenshospital.org
{kind=link}
{kind=link}